Indication
Coronary artery disease is a narrowing or blockage of one or more coronary arteries caused by fat deposits on the vessel wall (atherosclerosis). This partially or completely prevents oxygen-rich blood from reaching the heart muscle and can cause symptoms such as chest pain (angina). In extreme cases, when part of the heart muscle no longer receives any blood and oxygen, a heart attack occurs.
Reasons to opt for coronary bypass surgery instead of a cardiological procedure via the groin or wrist (such as balloon dilatation or stent placement) include the location and/or severity of the lesion, the anatomy of the coronary arteries and any associated medical problems (such as valve disease) that require heart surgery.
For some patients, a coronary bypass operation is combined with stent placement before or afterwards. This decision is always taken in consultation with the interventional cardiologists.
Course of the operation
Coronary bypass surgery is performed frequently. The operation carries a low risk, except in patients with multiple other medical problems or those operated on urgently after a heart attack. The procedure takes on average 4–6 hours and is carried out under general anaesthesia. The duration, set-up and course of the operation vary according to the type of surgery.
Conventional coronary bypass surgery
- During a conventional coronary bypass operation, or coronary artery bypass grafting (CABG), the chest is opened by means of a sternotomy (opening the breastbone along the midline).
- The heart-lung machine then temporarily takes over the function of the heart and lungs so that the heart can be stopped.
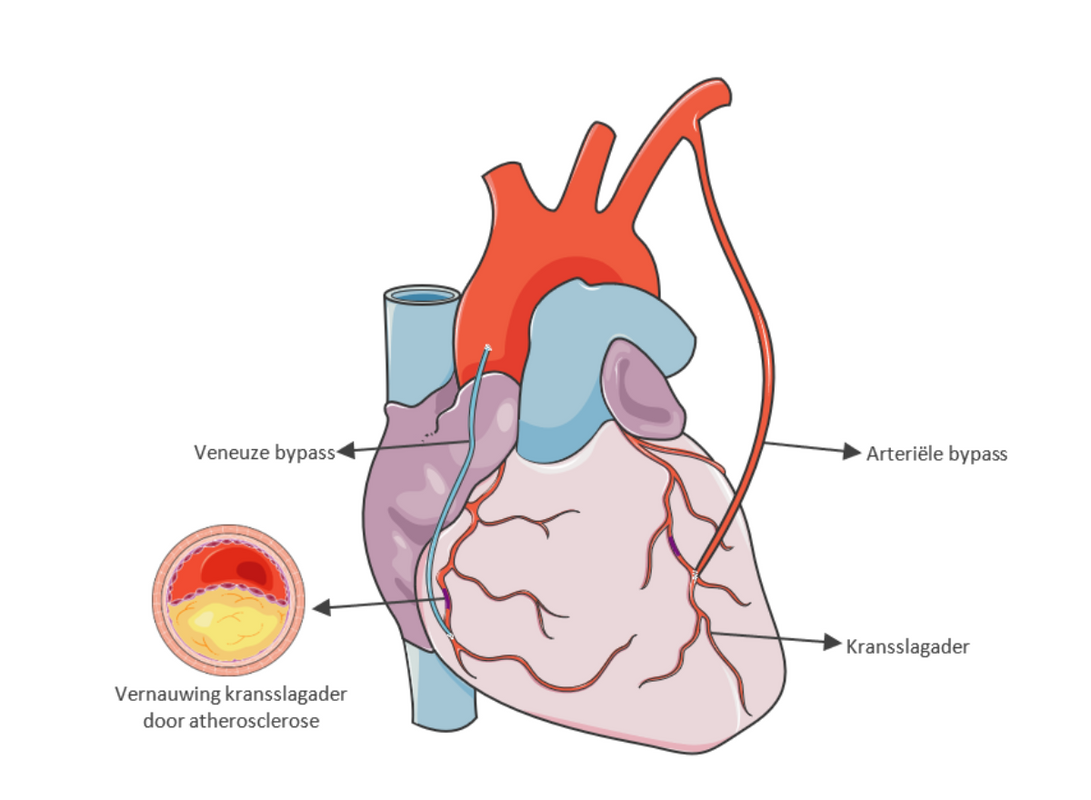
- The bypass is created using a healthy blood vessel from your body. Usually one or two arteries from the inside of the breastbone are used (arterial bypass), sometimes combined with a vein from the leg (venous bypass). This restores an adequate supply of oxygen-rich blood to the heart muscle.
- Once the bypass grafts have been sewn in place successfully, the heart-lung machine can be switched off. Blood then flows through your coronary arteries and your heart starts beating again.
Operation without heart-lung machine
Today, most of our bypass operations are performed on a beating heart, without using the heart-lung machine. This technique is called off-pump coronary artery bypass or OPCAB. While the bypass is being sewn in, the heart is locally stabilised but continues to pump.
Did you know that UZ Leuven is a leader in bypass operations without a heart-lung machine? Worldwide, only about 30% of bypass operations are performed on a beating heart.
Since 1999, more than 95% of bypass operations at UZ Leuven have been carried out without using the heart-lung machine.
Bypass surgery with the aid of the surgical robot
A variant of the OPCAB procedure is the minimally invasive direct coronary artery bypass or MIDCAB procedure. Here, the bypasses are created with the aid of the surgical robot on a beating heart.
In this procedure, the breastbone is not opened (no sternotomy); instead, a small incision is made between the ribs on the left side of the chest (mini-thoracotomy). A MIDCAB procedure is only possible when the front and/or side wall of the heart needs to be reached.
.png?style=W3sicmVzaXplIjp7ImZpdCI6Imluc2lkZSIsIndpZHRoIjoxNDIwLCJoZWlnaHQiOjEwODAsIndpdGhvdXRFbmxhcmdlbWVudCI6dHJ1ZX19XQ==&sign=e6e4a52591d4ee9665fb46d3d9aa804f6b3e8f4adef05b6ff048fb895affc126)
More about how your operation is carried out
Click here for more information about how heart surgery is performed.
Appointments
-
+32 16 34 42 60 - weekdays from 08:30 to 12:00 and 13:00 to 16:30


