Indication
Congenital diaphragmatic hernia (CDH) occurs when there is a gap in the muscle (the diaphragm) that divides the chest from the abdomen. Through this opening, the bowel, stomach and liver can enter the chest and compress the developing lungs, causing breathing problems and high blood pressure in the lungs after birth.
Despite the best neonatal care, CDH remains fatal in 30% of otherwise healthy babies.
Course of the treatment
During the procedure
The operation is done with local anesthesia for the mother and also pain relief for the fetus.
- The surgeon inserts a tiny camera into the womb through a 3-mm cut in the pregnant mother’s belly.
- The camera is inserted into the baby’s windpipe (trachea).
- A small balloon is inflated in the windpipe to block the fluid the lungs produce during pregnancy.
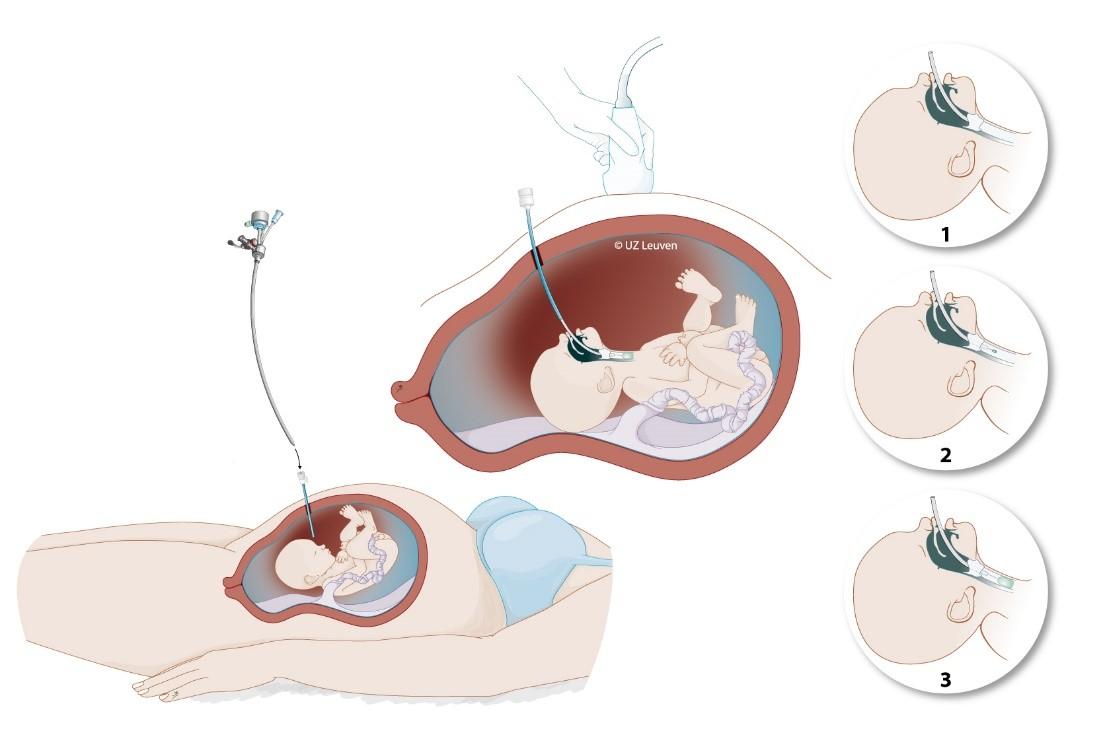
Illustration of the fetal surgery procedure in babies with congenital diaphragmatic hernia. A very small camera is inserted into the womb and then into the baby’s windpipe (trachea), to guide the positioning of a small balloon. The balloon is removed again before birth.
After the procedure
Temporarily blocking the windpipe leads to a build-up of the fluid in the lungs, which stimulates their growth. When the lungs grow, survival chances increase.
Toward the end of pregnancy, the surgeon removes the balloon so that the lungs can mature and the airways are free to breathe after birth.
Results
A randomised clinicial trial provided evidence that the FETO procedure benefits unborn babies with severe CDH. This type of clinical study is the golden standard, as patients are randomly assigned by a computer into a treatment and control group.
In babies with severe left-sided diaphragmatic hernia, i.e. those who have a less than 15% survival rate, FETO more than doubles the survival chances to 40%. The study also demonstrated a similar benefit in the rarer, right-sided form.
In the more moderate cases, i. e. babies who have a 50% chance to survive, FETO also tends to improve survival, but the gain is smaller.
Safety
When performed by experienced surgeons, FETO is safe for the mother and unborn baby. A disadvantage of fetal surgery is the need for a small opening in the womb, putting the mother at risk for membrane rupture, which may trigger premature birth. Premature birth can attenuate the positive effect of fetal surgery.
In addition, as long as the balloon is in place, mothers have to stay near the fetal surgery centre to be able to safely remove the balloon at all times.
The University Hospitals Leuven offer a comprehensive expert prenatal assessment of fetuses with CDH. It also has the world’s largest experience with fetal surgery for this condition, which may benefit selected fetuses. Fetal surgery adds to the care that neonatologists and surgeons provide after birth.